CJC-1295 (no DAC), Ipamorelin 10mg (Blend): Dosage, Benefits
CJC-1295 (no DAC), Ipamorelin 10mg (Blend)
Research Only
Growth Hormone Secretagogue
growth hormone stimulationresearch on GH pulsatilitystudy of receptor cross-talk
Last reviewed 03-2026·MyPeptideMatch Team
What Is the CJC-1295 (No DAC) / Ipamorelin Blend?
Two peptides working two different receptors at the same time — that's the core idea behind this blend. CJC-1295 (no DAC) hits the growth hormone-releasing hormone (GHRH) receptor to drive GH synthesis, while Ipamorelin activates the ghrelin receptor (GHS-R1a) to amplify the resulting pulse. The combination produces a GH release that's both larger and more physiologically timed than either compound achieves alone.
This is one of the most commonly discussed peptide combinations in the anti-aging and hormone optimization space, which is why it shows up constantly in clinic menus and research forums. That popularity is worth understanding in context: the evidence base here is largely preclinical and practitioner-reported. There are no published randomized controlled trials on this specific blend. What exists is mechanistic research on each component separately, animal studies, and a substantial body of practitioner experience — which is meaningful but not the same thing as Phase 3 human trial data.
The 10mg designation refers to the total peptide content in a blended vial — typically 5mg of each component — formulated for reconstitution and subcutaneous injection.
Key Takeaways
This blend combines two mechanistically distinct growth hormone secretagogues that work synergistically: CJC-1295 (no DAC) via GHRH receptors and Ipamorelin via ghrelin receptors (GHS-R1a).
Neither peptide is FDA-approved; both are classified as research-use-only in the United States and are not legally available through compounding pharmacies for human use under current FDA guidance.
Clinical evidence is preclinical — human data comes from practitioner reports and community consensus, not published RCTs on this specific blend.
The most commonly reported side effects reflect elevated GH and IGF-1 activity: water retention, joint discomfort, paresthesia, and transient flushing.
CJC-1295 (no DAC) has a short half-life of roughly 30 minutes, which means it produces a discrete GH pulse rather than sustained elevation — a key distinction from CJC-1295 with DAC.
100–300 mcg of each peptide per injection — dosing has not been established in human clinical trials; practitioner use reports range from 100–300 mcg per injection, but this lacks peer-reviewed validation.
CJC-1295 (no DAC) Half-life
~30 minutes
Ipamorelin Half-life
~2 hours — though ipamorelin half-life in humans is not established; preclinical data suggests approximately 2 hours, but clinical verification is lacking
Neither CJC-1295 (no DAC) nor Ipamorelin is FDA-approved, and neither is currently available through licensed compounding pharmacies for human clinical use under FDA guidance on bulk drug substances. Both are classified as research-use-only compounds. Any product labeled for human use is operating outside current US regulatory boundaries. The FDA has taken enforcement action against companies marketing unapproved peptide products; patients and providers should consult FDA.gov and the FDA's MedWatch program for current enforcement activity.
Typical Dosing — Practitioner & Community Ranges
There are no published clinical trials establishing an official dose for this specific CJC-1295 (no DAC) / Ipamorelin blend. The ranges below reflect what practitioners and researchers commonly reference, based on available protocol guides and community consensus.
Not clinical dosing
These ranges are not derived from randomized clinical trials. They represent practitioner and community consensus only. Dosing should be discussed with a licensed healthcare provider familiar with peptide research.
The most frequently cited approach uses 100–300 mcg of each peptide per injection, administered subcutaneously once daily — most often at night before sleep, timed to align with the body's natural nocturnal GH pulse.[1] Some protocols split this into two daily injections: one in the morning (fasted) and one at night. The rationale for nighttime dosing is straightforward: GH secretion is naturally highest in the first few hours of sleep, and co-administering both peptides at that window is thought to amplify rather than override the body's own rhythm.
Practitioner-Referenced Dosing Ranges by Goal
Parameter
Conservative
Moderate
Higher Research
CJC-1295 (no DAC) per injection
100 mcg
200 mcg
300 mcg
Ipamorelin per injection
100 mcg
200 mcg
300 mcg
Frequency
Once daily (PM)
Once daily (PM)
Twice daily
Evidence basis
Practitioner-reported, no clinical trial data available
Practitioner-reported, no clinical trial data available
Practitioner-reported, no clinical trial data available
Fasting for at least 90 minutes before injection is commonly recommended because elevated insulin suppresses GH release — eating right before an injection partially blunts the effect you're trying to achieve.[1] Injection sites are typically rotated across the abdomen, thigh, and lateral hip to prevent localized tissue changes.
Cycle length in practitioner protocols varies widely — anywhere from 8 weeks on with a 4-week break, to continuous low-dose use. There is no clinical trial data to guide this decision. practitioner-reported, not confirmed in published clinical trials
What Makes This Blend Different
Most growth hormone secretagogues work through one receptor. This combination works through two — and that's not a minor distinction. GHRH analogs like CJC-1295 (no DAC) tell the pituitary to synthesize and release GH. Ghrelin receptor agonists like Ipamorelin tell the pituitary to release GH through a completely separate signaling pathway. When you activate both simultaneously, the GH pulse is substantially larger than either compound produces alone — a synergy that has been documented in animal research and is the mechanistic basis for why this combination became popular in the first place.[2]
Why 'no DAC' matters
CJC-1295 comes in two versions. The DAC (Drug Affinity Complex) version binds to albumin in the bloodstream, extending its half-life to roughly 8 days and producing sustained, blunted GH elevation. CJC-1295 without DAC has a half-life of approximately 30 minutes — it produces a discrete, pulsatile GH release that more closely mimics natural physiology. Most practitioners prefer the no-DAC version for this reason: chronic GH elevation carries different risk considerations than pulsatile release, and the pulsatile pattern is how the body normally operates.
Ipamorelin also has a selectivity profile that distinguishes it from older ghrelin mimetics like GHRP-6 and GHRP-2. Those compounds stimulate GH release but also significantly raise cortisol and prolactin — hormones you generally don't want elevated.[3] Ipamorelin produces a much more selective GH pulse with minimal cortisol or prolactin stimulation, which is why it became the preferred ghrelin-receptor agonist in most modern research protocols.[3]
How Does This Blend Work?
The growth hormone axis runs on a push-pull system. The hypothalamus releases GHRH (growth hormone-releasing hormone), which signals the pituitary gland to produce and release GH. Somatostatin, also from the hypothalamus, acts as the brake — it suppresses GH release. Ghrelin, produced mainly in the stomach, hits a separate receptor on pituitary cells and amplifies GH release through calcium signaling while simultaneously suppressing somatostatin's braking effect.
CJC-1295 (no DAC) is a modified analog of GHRH. Its amino acid sequence is based on the first 29 amino acids of native GHRH (GHRH 1-29), with substitutions that improve stability and receptor binding without dramatically extending half-life.[4] When it binds to GHRH receptors on pituitary somatotroph cells, it activates adenylyl cyclase, raises intracellular cyclic AMP (cAMP), and drives GH synthesis and release.[4]
Ipamorelin is a pentapeptide (five amino acids: Aib-His-D-2-Nal-D-Phe-Lys-NH₂) that selectively binds the ghrelin receptor, also known as GHS-R1a.[3] Receptor activation triggers a calcium-dependent signaling cascade inside pituitary cells that independently drives GH secretion. Critically, Ipamorelin does this without meaningfully raising ACTH, cortisol, or prolactin — a selectivity profile that distinguishes it from earlier GH secretagogues.[3]
When both peptides are injected together, they hit the pituitary from two different angles at the same time. The result is a GH pulse that's larger than either compound produces alone — synergy that's been confirmed in animal studies.[2] That pulse then triggers the liver to produce IGF-1 (insulin-like growth factor 1), which is the downstream mediator responsible for most of the tissue-level effects associated with GH: muscle protein synthesis, fat metabolism, connective tissue repair, and cellular recovery.
What the Clinical Evidence Actually Shows
This is where honest context matters. The mechanistic story is well-supported. The human clinical evidence for this specific blend is not.
CJC-1295 (no DAC) — the component evidence: The underlying GHRH 1-29 analog (Sermorelin) has been studied in humans and shown to stimulate GH release in a pulsatile, dose-dependent manner.[5] Studies on modified GHRH analogs confirm that structural modifications preserving the first 29 amino acids maintain receptor binding and biological activity.[4] A study by Ionescu and Frohman published in the Journal of Clinical Endocrinology & Metabolism characterized the pharmacokinetics and GH-stimulating effects of GHRH analogs, establishing the mechanistic foundation for compounds in this class.[4]
Ipamorelin — the component evidence: Raun et al. (1998) published the foundational characterization of Ipamorelin in European Journal of Endocrinology, establishing its selectivity for GHS-R1a and its GH-stimulating profile in animal models.[3] That study specifically compared Ipamorelin to GHRP-6 and GHRP-2, demonstrating the superior selectivity profile — the cortisol and prolactin sparing — that makes Ipamorelin the preferred compound in this class.[3]
The synergy evidence: Bowers (2001) and subsequent preclinical work documented that combined GHRH and ghrelin receptor activation produces supra-additive GH release — the mechanistic basis for combining these two compound classes.[2] This synergy has been replicated in animal models but, while preclinical research on GHRH and ghrelin receptor agonist combinations exists in the literature, the specific synergy evidence for this CJC-1295 (no DAC) + Ipamorelin 10mg blend formulation has not been established in human clinical trials and no peer-reviewed dose-finding studies exist for this combination product.
The honest gap: There is no published randomized controlled trial on the CJC-1295 (no DAC) / Ipamorelin combination in humans. The clinical rationale is mechanistically sound and supported by component-level data, but the blend itself has not been evaluated for efficacy or safety in a formal human trial.
What the Evidence Does Not Show
Efficacy in humans from RCT data — No published randomized controlled trial has tested this specific blend in human subjects. Practitioner reports and community data fill this gap, but they are not a substitute for controlled trial evidence.
Optimal dosing in humans — Every dose range cited for this blend is derived from practitioner consensus, not a dose-finding trial. The "right" dose for a given individual is genuinely unknown from a clinical evidence standpoint.
Long-term safety — There is no long-term safety data on chronic use of this combination. GH axis manipulation over months or years carries theoretical risks — including effects on insulin sensitivity and IGF-1-related cellular proliferation — that have not been formally evaluated for this blend.
Body composition outcomes from controlled trials — Practitioner reports of fat loss and muscle gain are plausible given the known effects of GH and IGF-1, but no controlled human trial has quantified these outcomes for this specific combination.
Cardiovascular outcomes — Unknown. No CV outcomes data exists for this blend or its components used in combination.
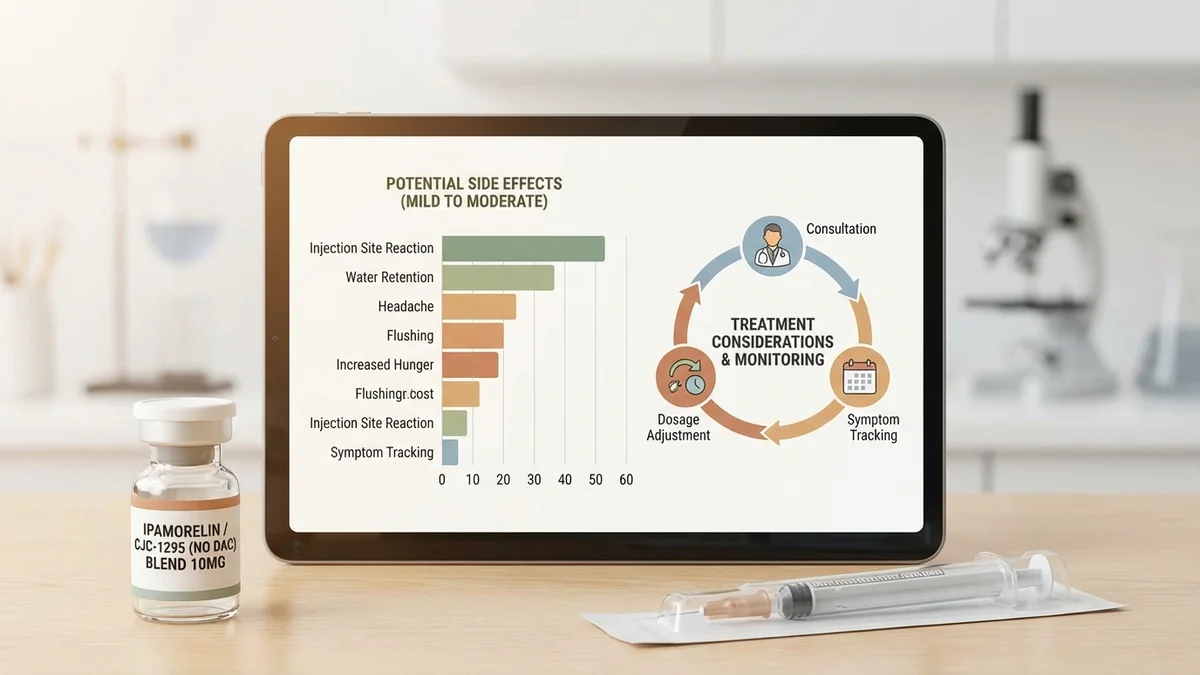
Side Effects — What to Actually Expect
The side effects of this blend reflect elevated GH and IGF-1 activity, along with the acute effects of ghrelin receptor activation. They're generally mild and dose-dependent, but worth knowing before you start.
Shortly after injection:
Flushing and warmth — a transient sensation that typically peaks within 10–20 minutes of injection and resolves on its own; more common with higher doses
Headache — reported by some users shortly after injection; usually mild and brief; adverse event profiles for this peptide blend have not been established in human clinical trials or published literature.
Tingling or paresthesia — a pins-and-needles sensation, particularly in the hands and face; reflects GH activity on peripheral nerves and typically diminishes as the body adjusts
With ongoing use:
Water retention — the most commonly reported effect; GH promotes sodium and water reabsorption, which can cause a bloated or puffy feeling, particularly in the first few weeks
Joint discomfort — mild aching in the hands, wrists, or knees; a known effect of elevated GH and IGF-1 on connective tissue; usually resolves with dose reduction
Injection site reactions — redness, mild swelling, or tenderness at the injection site; rotating sites across the abdomen, thigh, and lateral hip reduces this significantly
Less common:
Transient hypoglycemia — GH can affect insulin sensitivity; some users report light-headedness or hunger shortly after injection, particularly if fasted — though this blend has no human clinical data, and while isolated GH secretagogues may theoretically affect glucose homeostasis, adverse effects in this specific combination have not been established in humans.
Increased hunger — Ipamorelin's ghrelin receptor activity can stimulate appetite, though this effect is generally milder with Ipamorelin than with GHRP-6
If you notice persistent joint pain, significant edema, or any signs of carpal tunnel syndrome (numbness and weakness in the hand), that's a signal to reduce dose or pause use and talk to a provider. Prolonged IGF-1 elevation is the likely mechanism, and the symptom typically resolves with dose reduction.
Regulatory & Access Status
Legal status in the United States — 2026-03
CJC-1295 (no DAC) and Ipamorelin are not FDA-approved for any indication. Both are classified as research-use-only compounds. Under current FDA guidance, they are not eligible for compounding by licensed pharmacies for human use. Products sold for human administration are operating outside US regulatory boundaries. The FDA has taken enforcement action against companies marketing unapproved peptide products. Consult FDA.gov and the FDA's MedWatch program for current enforcement activity.
The practical reality: this blend circulates in the US primarily through research chemical vendors and, in some cases, through clinics operating in regulatory gray areas. The 2023–2024 FDA enforcement wave targeting compounding pharmacies significantly reduced the availability of this and related peptides through what had previously been a common access pathway — licensed compounding under 503A. That pathway is no longer viable for these compounds under current agency guidance.
If you're seeing this blend offered by a telehealth clinic or compounding pharmacy, that provider is taking on meaningful regulatory risk, and you should understand that context before proceeding.
Sourcing & Safety
If you're going to source this compound through research chemical channels — and many people will regardless — here's what separates a safer purchase from a dangerous one.
What to look for:
Third-party Certificate of Analysis (COA) — should be from an independent analytical laboratory, not the vendor's own in-house testing. The COA should confirm peptide identity, purity, and the absence of common contaminants.
HPLC purity report showing ≥98% — high-performance liquid chromatography is the standard method for peptide purity verification. Anything below 98% is a quality concern.
Mass spectrometry confirmation — confirms the peptide's molecular weight matches the expected sequence. This catches substitution errors that HPLC alone won't catch.
Lyophilized (freeze-dried) powder — the stable storage form. Pre-mixed or pre-dissolved products raise immediate quality and sterility questions.
Bacteriostatic water for reconstitution — not sterile water, not tap water. Bacteriostatic water contains 0.9% benzyl alcohol, which inhibits bacterial growth in the vial after reconstitution.
Red flags:
No COA or "in-house testing only" — the single most common sign of a low-quality vendor. Walk away.
Price significantly below market — real peptide synthesis and independent testing cost money. Prices that seem too good are usually accurate.
Pre-mixed vials or liquid peptides — peptides in solution degrade faster and carry higher contamination risk than lyophilized powder.
No clear labeling of peptide content per vial — if the vendor can't tell you exactly how much CJC-1295 and Ipamorelin are in the vial, that's a problem.
Reconstitute with bacteriostatic water, use insulin syringes (typically 29–31 gauge, 0.5 inch), and store reconstituted vials refrigerated at 2–8°C. Discard unused reconstituted product after 30 days.
FAQ
What's the difference between CJC-1295 with DAC and without DAC?
The DAC (Drug Affinity Complex) modification causes CJC-1295 to bind to albumin in the bloodstream, extending its half-life to approximately 8 days and producing sustained GH elevation. Without DAC, the half-life is roughly 30 minutes, producing a discrete GH pulse that mirrors natural pulsatile secretion. Most practitioners prefer the no-DAC version because chronic GH elevation carries different risk considerations than pulsatile release.
Why is Ipamorelin preferred over GHRP-6 for this type of protocol?
Both are ghrelin receptor agonists, but GHRP-6 significantly raises cortisol and prolactin alongside GH — hormones most people don't want elevated.[3] Ipamorelin produces a much more selective GH pulse with minimal effect on cortisol or prolactin, making it a cleaner option for GH axis research.[3] GHRP-6 also tends to produce stronger appetite stimulation.
Can you take CJC-1295 and Ipamorelin separately instead of as a blend?
Yes. The blend is simply a convenience formulation — both peptides in one vial. Some practitioners prefer separate vials for flexibility in dosing each component independently. The pharmacology is identical whether you inject them together or separately within a short window.
How should this blend be stored after reconstitution?
Reconstituted vials should be refrigerated at 2–8°C and kept away from light. Most practitioners recommend discarding unused reconstituted product after 30 days. Lyophilized (unreconstituted) powder is more stable and can typically be stored at room temperature short-term or refrigerated long-term, though specific stability data for this blend is limited. Storage and stability recommendations for reconstituted CJC-1295 (no DAC) and Ipamorelin blends are not established in published clinical or regulatory data; practitioners should follow manufacturer guidance and consult qualified healthcare professionals regarding product handling.
Is this blend detectable on sports drug tests?
GH secretagogues including GHRP and GHRH analogs are prohibited by the World Anti-Doping Agency (WADA) under the category of peptide hormones, growth factors, and related substances.[6] Detection methods for these compounds in urine and blood continue to improve. If you compete in any sport governed by WADA or USADA rules, this compound is prohibited.
Related Peptides & Comparisons
If you're researching this blend, a few related compounds are worth understanding in context. Sermorelin is the closest approved analog — it's the original GHRH 1-29 peptide that CJC-1295 (no DAC) is derived from, and it has a longer history of clinical use in GH deficiency research. Tesamorelin is an FDA-approved GHRH analog (for HIV-associated lipodystrophy) that provides the clearest picture of what controlled human trials on GHRH analogs actually show.
On the ghrelin receptor side, MK-677 (Ibutamoren) is an oral ghrelin mimetic that activates the same GHS-R1a receptor as Ipamorelin but with a much longer half-life — around 24 hours — and without the need for injection. It's worth understanding the tradeoffs between these approaches if you're researching GH axis optimization.
GH Secretagogue Comparison
Parameter
CJC-1295/Ipamorelin
Sermorelin
MK-677
Receptor target
GHRH-R + GHS-R1a
GHRH-R
GHS-R1a
Administration
Subcutaneous injection
Subcutaneous injection
Oral
GH pulse type
Pulsatile
Pulsatile
Sustained elevation
FDA status
Research only
Research only
Research only
Human RCT data
None (blend)
Limited
Limited
Half-life
~30 min / ~2 hr
~10–20 min
~24 hr
References
Walker RF. "Sermorelin: A better approach to management of adult-onset growth hormone insufficiency?" Clinical Interventions in Aging. 2006;1(4):307–308. PMID: 18046908
Raun K, Hansen BS, Johansen NL, et al. "Ipamorelin, the first selective growth hormone secretagogue." European Journal of Endocrinology. 1998;139(5):552–561. PMID: 9849822
Ionescu M, Frohman LA. "Pulsatile secretion of growth hormone (GH) persists during continuous stimulation by CJC-1295, a long-acting GH-releasing hormone analog." Journal of Clinical Endocrinology & Metabolism. 2006;91(12):4792–4797. PMID: 16984990
Vittone J, Blackman MR, Busby-Whitehead J, et al. "Effects of single nightly injections of growth hormone-releasing hormone (GHRH 1-29) in healthy elderly men." Metabolism. 1997;46(1):89–96. PMID: 9005976
World Anti-Doping Agency. "Prohibited List 2024: Section 2 — Peptide Hormones, Growth Factors, Related Substances and Mimetics." WADA. 2024. Available at: wada-ama.org
This content is for informational purposes only and does not constitute medical advice. Consult a licensed healthcare provider before starting any treatment.
Find Clinics Offering CJC-1295 (no DAC), Ipamorelin 10mg (Blend)
2 clinics in our directory offer CJC-1295 (no DAC), Ipamorelin 10mg (Blend). Use the button below to find one near you.
MyPeptideMatch.com does not provide medical advice. Always consult a qualified healthcare provider before starting any peptide therapy. Regulatory status may change.