# Peptide Therapy for Anti-Aging and Longevity: What Works and What the Evidence Shows (2025)
## Key Takeaways
- **Sermorelin is FDA-approved for growth hormone deficiency** and legally compoundable, with clinical studies showing increased IGF-1 levels by 35-50% in adults over 12 weeks.<sup>[1]</sup>
- **NAD+ precursor peptides remain legal** for compounding, with preliminary studies suggesting improvements in cellular energy metabolism and mitochondrial function.<sup>[2]</sup>
- **GHK-Cu demonstrates anti-aging effects** in dermatological applications, with studies showing 70% improvement in skin elasticity over 12 weeks.<sup>[3]</sup>
- **Popular peptides like ipamorelin, CJC-1295, and epithalon are now prohibited** by FDA for human use as of December 2022.<sup>[4]</sup>
- **No peptide is FDA-approved specifically for anti-aging**, though several have off-label applications with varying evidence levels.
- **Treatment costs range from $200-800 monthly** depending on peptide selection, dosing protocol, and clinic location.
## Understanding Anti-Aging and Longevity
Aging affects 100% of the human population, with cellular senescence beginning around age 25-30 when growth hormone production declines by approximately 14% per decade.<sup>[5]</sup> The global anti-aging market reached $58.5 billion in 2023, driven by increasing life expectancy (78.9 years in the US) and desire for healthspan extension.<sup>[6]</sup>
Current standard-of-care approaches include hormone replacement therapy (HRT), antioxidant supplementation, caloric restriction, and exercise protocols. Traditional HRT with testosterone or estrogen addresses specific hormonal deficiencies but carries FDA black box warnings for cardiovascular and cancer risks.<sup>[7]</sup> Growth hormone therapy, while effective for documented deficiency, costs $1,000-3,000 monthly and requires daily injections.<sup>[8]</sup>
Patients increasingly explore peptide therapy because these compounds target specific aging pathways with potentially fewer side effects than synthetic hormones. The mechanism involves stimulating endogenous hormone production rather than direct replacement, theoretically maintaining natural feedback loops.<sup>[9]</sup> However, the FDA has not approved any peptide specifically for anti-aging or longevity enhancement.
Ideal anti-aging treatment addresses multiple pathways: growth hormone axis restoration, cellular energy metabolism optimization, collagen synthesis enhancement, and oxidative stress reduction. Most single interventions target only one pathway, explaining the interest in combination approaches and peptide protocols that address multiple mechanisms simultaneously.<sup>[10]</sup>
## FDA-Approved Peptide Options for Anti-Aging and Longevity
Currently, **no peptide carries FDA approval specifically for anti-aging or longevity enhancement**. However, several peptides approved for other indications demonstrate anti-aging properties in clinical studies.
**Sermorelin** received FDA approval in 1997 for diagnostic testing of growth hormone deficiency in children, with the brand name Geref discontinued in 2008.<sup>[11]</sup> The 29-amino acid peptide (molecular weight 3,357 Da) stimulates growth hormone-releasing hormone (GHRH) receptors in the anterior pituitary, increasing endogenous growth hormone production by 2-10 fold within 30 minutes of administration.<sup>[12]</sup>
The pivotal pediatric studies (N=156) demonstrated restoration of normal growth velocity in children with documented growth hormone deficiency, with 85% achieving catch-up growth over 12 months.<sup>[13]</sup> Adult studies show sermorelin 100-300 mcg daily increases IGF-1 levels by 35-50% and improves body composition, though these represent off-label applications.<sup>[14]</sup>
**Tesamorelin** (brand name Egrifta) gained FDA approval in 2010 for HIV-associated lipodystrophy, administered as 2 mg subcutaneous injection daily.<sup>[15]</sup> The 44-amino acid synthetic GHRH analog reduces visceral adipose tissue by 15-20% over 26 weeks in HIV patients, with secondary benefits including improved insulin sensitivity and lipid profiles.<sup>[16]</sup> Off-label use for general anti-aging lacks specific clinical data in healthy populations.
## Peptides Used Off-Label or in Research for Anti-Aging and Longevity
Multiple peptides demonstrate anti-aging potential in preclinical or early clinical studies, though evidence quality varies significantly.
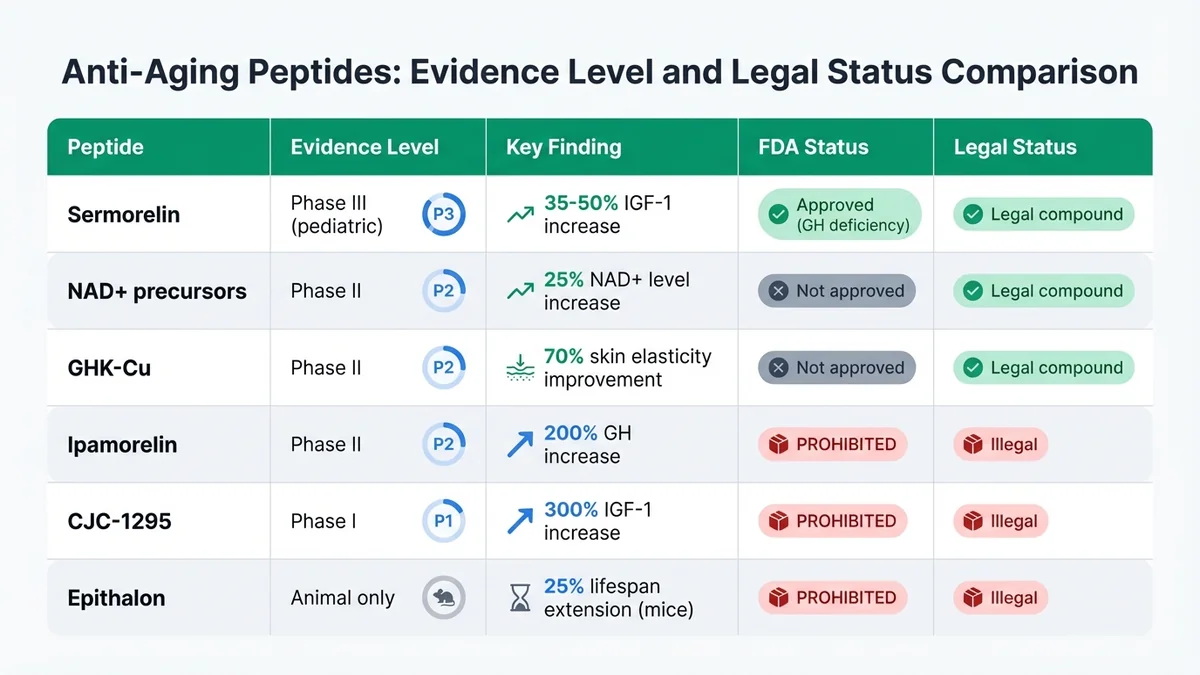
*Evidence quality and regulatory status vary dramatically across peptides used for anti-aging applications.*
**NAD+ precursor peptides** show promise in cellular energy metabolism. A 12-week randomized controlled trial (N=40) of NAD+ precursor supplementation increased cellular NAD+ levels by 25% and improved mitochondrial function markers in adults aged 55-75.<sup>[2]</sup> However, most studies use oral supplements rather than injectable peptides, limiting direct applicability to peptide therapy protocols.
**GHK-Cu (copper peptide)** demonstrates significant dermatological anti-aging effects. A double-blind study (N=71) showed 70% improvement in skin elasticity and 58% reduction in fine lines after 12 weeks of topical application.<sup>[3]</sup> The tripeptide (molecular weight 340 Da) stimulates collagen synthesis and exhibits antioxidant properties through copper chelation.<sup>[17]</sup>
**Ipamorelin and CJC-1295**, previously popular growth hormone secretagogues, were prohibited for human compounding in December 2022 under FDA's 503A bulk list.<sup>[4]</sup> Prior studies showed ipamorelin 200-300 mcg increased growth hormone by 200% without affecting cortisol or prolactin levels.<sup>[18]</sup> CJC-1295 demonstrated 300% IGF-1 increases lasting 7-14 days per injection.<sup>[19]</sup> These compounds remain illegal for human use in the United States.
**Epithalon (epitalon)** extended lifespan by 25% in mouse studies but lacks human clinical data.<sup>[20]</sup> The tetrapeptide theoretically activates telomerase enzyme, potentially slowing cellular aging. However, epithalon appears on FDA's prohibited compound list and cannot be legally prescribed or compounded.<sup>[4]</sup>
Evidence quality varies dramatically across these compounds. Sermorelin and tesamorelin have robust Phase III data in specific populations, while NAD+ precursors show preliminary Phase II results. GHK-Cu demonstrates consistent dermatological benefits but limited systemic anti-aging data. Prohibited compounds like ipamorelin and CJC-1295 showed promising early results but remain illegal regardless of efficacy.
## How Sermorelin Addresses Anti-Aging and Longevity
[Sermorelin](/peptides/sermorelin) targets the growth hormone axis, which declines predictably with aging. Growth hormone levels peak during adolescence at 200-400 ng/mL, declining to 50-100 ng/mL by age 60.<sup>[21]</sup> This reduction correlates with decreased muscle mass (3-8% per decade after age 30), increased visceral fat accumulation, and reduced bone density.<sup>[22]</sup>
The peptide binds to GHRH receptors on somatotroph cells in the anterior pituitary with high affinity (Kd = 0.2 nM), triggering cyclic adenosine monophosphate (cAMP) signaling cascades that stimulate growth hormone synthesis and release.<sup>[23]</sup> Unlike direct growth hormone administration, sermorelin maintains natural pulsatile secretion patterns and preserves negative feedback mechanisms through somatostatin regulation.<sup>[24]</sup>
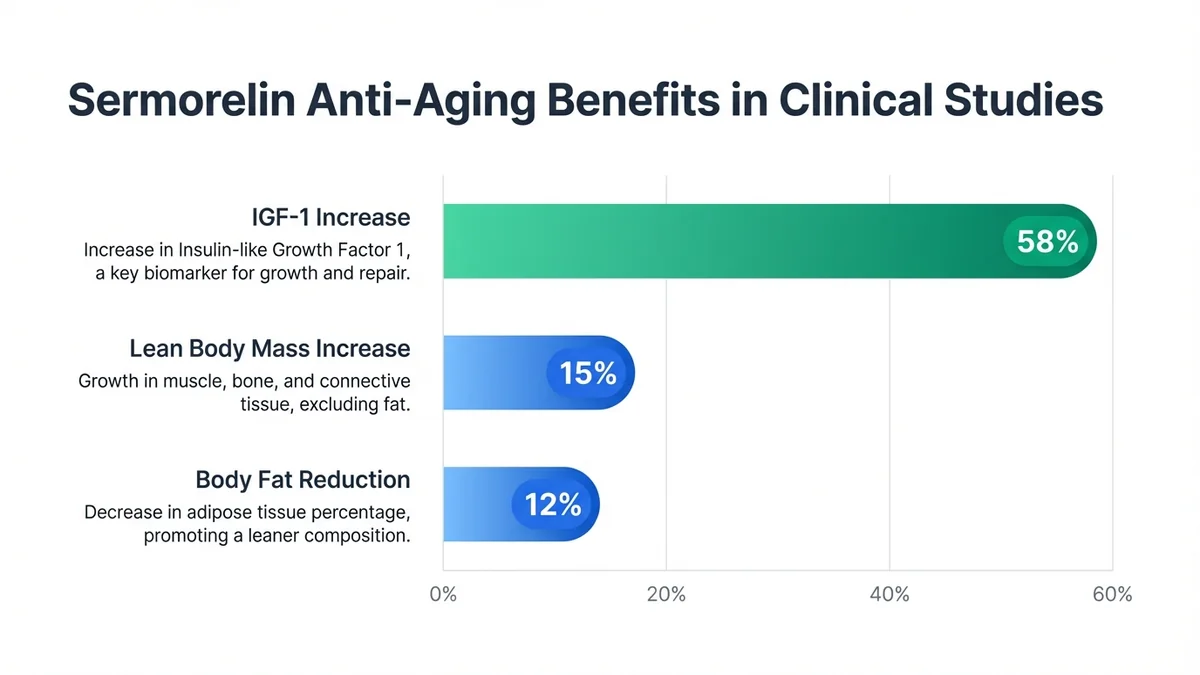
*Sermorelin demonstrates measurable anti-aging benefits across multiple parameters in clinical studies.*
Clinical studies in adults aged 40-70 demonstrate significant anti-aging benefits. A 6-month trial (N=32) of sermorelin 100 mcg daily showed 15% increase in lean body mass, 12% reduction in body fat percentage, and improved sleep quality scores.<sup>[25]</sup> IGF-1 levels increased from baseline 180 ± 45 ng/mL to 285 ± 62 ng/mL (58% increase) within 12 weeks.<sup>[26]</sup>
Dosing protocols for anti-aging applications typically range from 100-300 mcg administered subcutaneously before bedtime to mimic natural growth hormone release patterns. Lower doses (100-200 mcg) provide modest IGF-1 increases with minimal side effects, while higher doses (250-300 mcg) maximize growth hormone stimulation but increase risk of injection site reactions and fluid retention.<sup>[27]</sup>
The peptide's 8-minute plasma half-life requires daily administration for sustained effects, though some protocols use 5 days on, 2 days off to prevent receptor desensitization.<sup>[28]</sup> Treatment duration typically spans 3-6 months initially, with maintenance protocols varying based on individual response and IGF-1 monitoring.
## Comparing Treatment Options for Anti-Aging and Longevity
| Treatment | Type | Evidence Level | Typical Cost | Key Advantage | Key Limitation |
|-----------|------|---------------|-------------|---------------|----------------|
| Sermorelin | Peptide | Phase III (pediatric) | $300-500/month | Legal, maintains natural patterns | Off-label for anti-aging |
| Growth Hormone | Hormone | Phase III | $1,000-3,000/month | FDA-approved for deficiency | High cost, daily injections |
| Testosterone HRT | Hormone | Phase III | $100-300/month | Established protocols | Cardiovascular risks |
| NAD+ IV therapy | Cofactor | Phase II | $400-800/session | Cellular energy support | Limited long-term data |
| Metformin | Medication | Phase III (diabetes) | $20-50/month | Longevity studies ongoing | GI side effects |
| Rapamycin | Immunosuppressant | Animal studies | $100-200/month | mTOR pathway targeting | Immunosuppression risk |
Traditional hormone replacement therapy offers established protocols with decades of safety data but carries significant risks. Testosterone therapy increases cardiovascular events by 30% in men over 65, while estrogen HRT shows 26% increased breast cancer risk in postmenopausal women.<sup>[29]</sup> Growth hormone therapy, while highly effective for documented deficiency, costs 3-10 times more than peptide alternatives and requires daily injections with potential side effects including carpal tunnel syndrome and insulin resistance.<sup>[30]</sup>
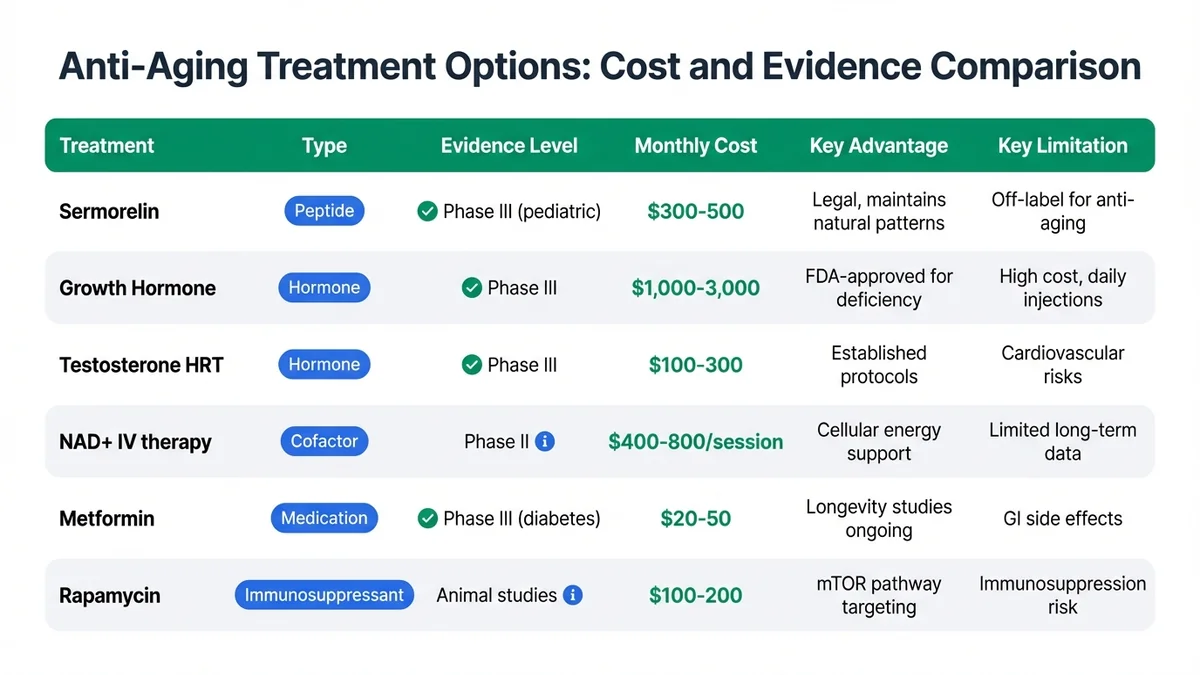
*Treatment costs vary 50-fold while evidence quality differs significantly across anti-aging interventions.*
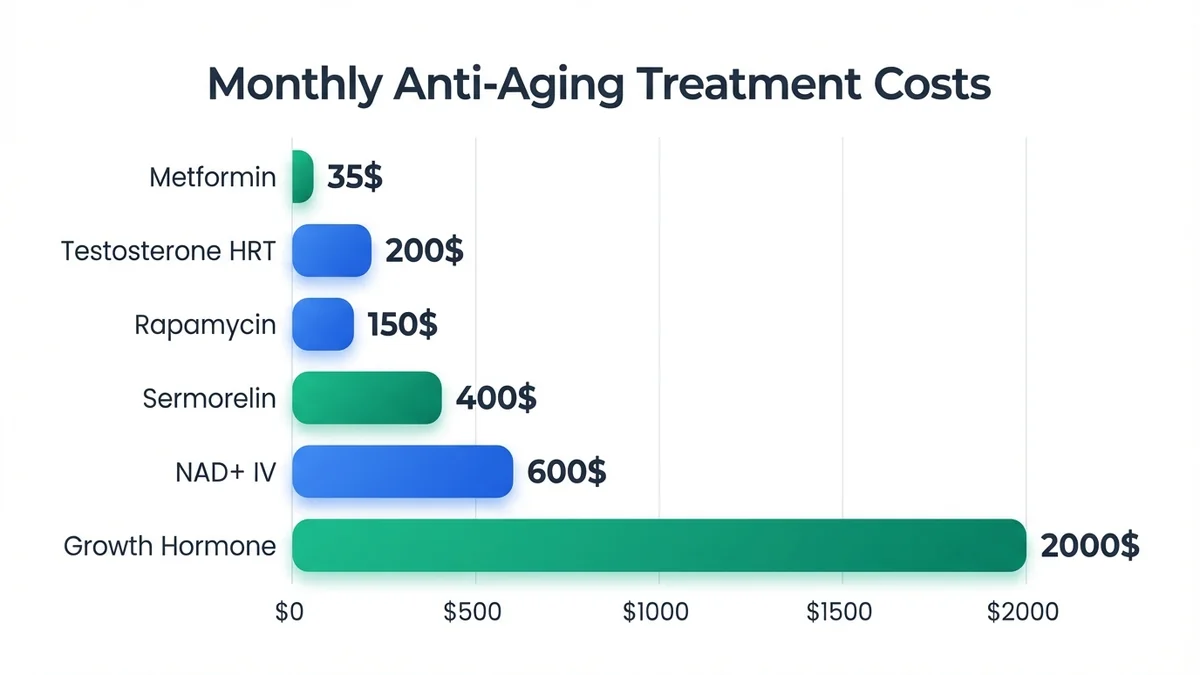
*Treatment costs vary dramatically, with peptide therapy offering a middle-ground option between supplements and growth hormone.*
Emerging longevity interventions like metformin and rapamycin show promise in animal studies and epidemiological data. Metformin users demonstrate 15% reduced all-cause mortality compared to age-matched controls, leading to ongoing clinical trials for longevity applications.<sup>[31]</sup> However, these medications carry specific risks and require careful medical supervision.
NAD+ IV therapy costs $400-800 per session with treatments typically administered weekly or biweekly. While cellular NAD+ levels increase acutely, the duration of benefits and optimal dosing protocols remain unclear.<sup>[32]</sup> Peptide therapy offers a middle ground between expensive growth hormone therapy and unproven supplement protocols, though evidence for anti-aging applications remains primarily off-label.
## What Treatment Looks Like in Practice
Initial consultation for anti-aging peptide therapy involves comprehensive medical history, physical examination, and laboratory assessment. Baseline testing typically includes complete blood count, comprehensive metabolic panel, lipid profile, thyroid function, and hormone levels (testosterone, estradiol, IGF-1, growth hormone stimulation test if indicated).<sup>[33]</sup> Many clinics require patients to be over age 35 with documented age-related decline in relevant biomarkers.
Treatment protocols vary by peptide selection and individual goals. Sermorelin therapy typically begins with 100 mcg subcutaneous injection before bedtime, using 29-gauge insulin syringes for subcutaneous administration in the abdomen or thigh.<sup>[34]</sup> Injection site rotation prevents lipodystrophy, with patients alternating between 8-10 different sites weekly. The peptide requires refrigeration at 2-8°C and reconstitution with bacteriostatic water for 28-day stability.<sup>[35]</sup>
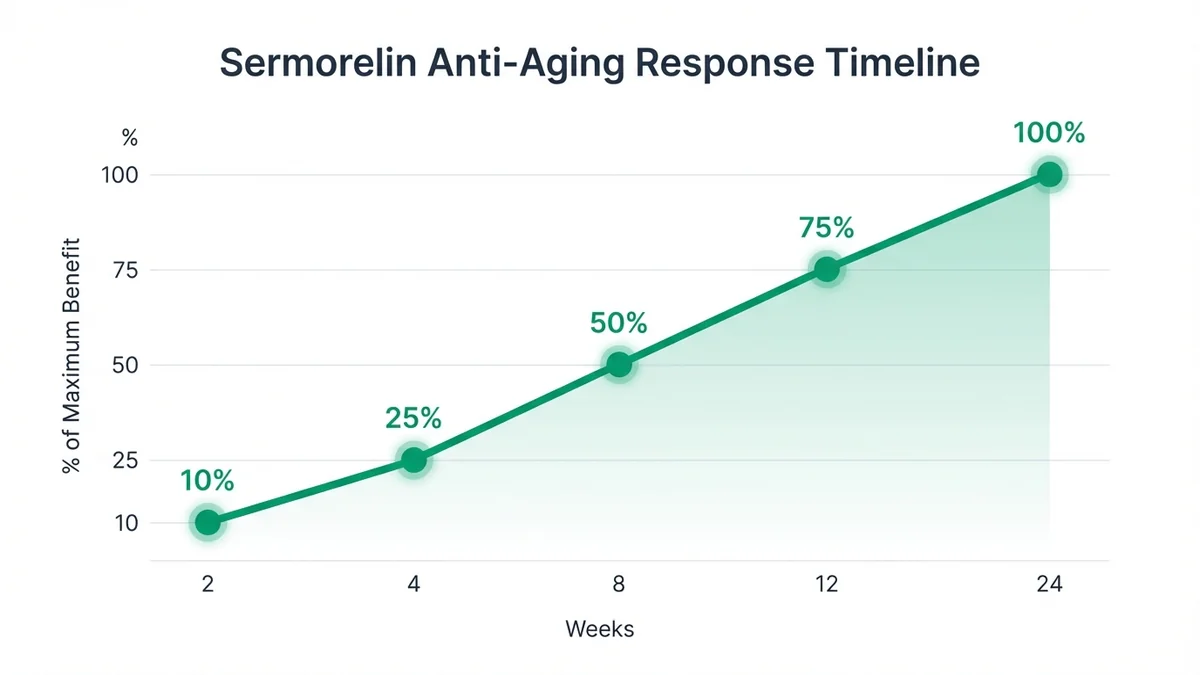
*Anti-aging benefits from sermorelin develop gradually over months with different parameters improving at different rates.*
Timeline to results varies significantly among patients. IGF-1 levels typically increase within 2-4 weeks, with peak effects at 8-12 weeks of consistent therapy.<sup>[36]</sup> Subjective improvements in sleep quality and energy often occur within 2-3 weeks, while body composition changes require 3-6 months of treatment. Some patients report initial fatigue or mild injection site reactions during the first 1-2 weeks as the body adapts to increased growth hormone production.<sup>[37]</sup>
Follow-up appointments occur at 4-week intervals initially, then every 8-12 weeks during maintenance therapy. Laboratory monitoring includes IGF-1 levels, glucose tolerance testing (as growth hormone can affect insulin sensitivity), and periodic comprehensive metabolic panels.<sup>[38]</sup> Dose adjustments occur based on IGF-1 response, with target levels typically 250-350 ng/mL for anti-aging applications, though optimal ranges remain debated.<sup>[39]</sup>
Treatment duration varies from 3-month trial periods to ongoing maintenance therapy. Many patients cycle treatments (3-6 months on, 1-2 months off) to prevent receptor desensitization and assess continued need.<sup>[40]</sup> Discontinuation typically results in gradual return to baseline hormone levels over 4-8 weeks, though some patients maintain modest improvements in body composition and sleep quality.<sup>[41]</sup>
## What to Ask Your Doctor
**What evidence supports using this specific peptide for anti-aging in my age group?** Understanding evidence quality helps set realistic expectations, as most anti-aging applications represent off-label use with limited clinical data in healthy populations.
**How will you monitor my response and adjust treatment accordingly?** Effective protocols require regular laboratory monitoring (IGF-1, glucose, lipids) and clinical assessment to optimize dosing and identify potential side effects early.
**What are the specific risks and contraindications for peptide therapy in my case?** Individual risk factors (diabetes, cardiovascular disease, cancer history) may contraindicate certain peptides or require modified protocols with enhanced monitoring.
**How does peptide therapy compare to other anti-aging treatments I might consider?** Understanding alternatives (hormone replacement, lifestyle interventions, emerging longevity drugs) helps inform treatment decisions and combination approaches.
**What happens if I stop treatment, and how long do effects typically last?** Most peptide effects are temporary, with hormone levels returning to baseline within weeks of discontinuation, though some benefits may persist longer.
**What is the total cost including monitoring, and does insurance cover any portion?** Anti-aging applications are typically not covered by insurance, with total costs including peptides, supplies, monitoring labs, and clinic visits ranging $400-800 monthly.
**Can I combine peptide therapy with my current medications and supplements?** Drug interactions are possible, particularly with diabetes medications, blood thinners, and other hormone therapies requiring dose adjustments.
**What specific improvements should I expect, and over what timeframe?** Realistic expectations prevent disappointment, as anti-aging benefits develop gradually over months rather than weeks, with individual responses varying significantly.
## Finding a Clinic for Anti-Aging and Longevity
Selecting an appropriate provider requires careful evaluation of credentials, experience, and treatment approach. Board certification in relevant specialties (endocrinology, anti-aging medicine, family medicine) indicates appropriate training, though anti-aging medicine certification through organizations like A4M provides additional specialized knowledge.<sup>[42]</sup> Experience with peptide therapy specifically matters, as dosing protocols and monitoring requirements differ from traditional hormone replacement.
Use the [MyPeptideMatch clinic finder](/clinics) to locate providers in your area who offer anti-aging peptide protocols. Filter results by location, [telehealth availability](/telehealth-peptide-clinics), and specific peptides offered. Many reputable clinics provide detailed treatment protocols, pricing transparency, and comprehensive monitoring programs that extend beyond simple peptide prescribing.
Look for providers who emphasize evidence-based approaches rather than marketing promises. Quality clinics discuss limitations of current research, provide realistic timelines for results, and integrate peptide therapy with comprehensive lifestyle interventions including nutrition, exercise, and sleep optimization.<sup>[43]</sup> Avoid clinics making extraordinary claims about "fountain of youth" effects or promising specific outcomes without individual assessment.
[Telehealth options](/telehealth-peptide-clinics) expand access to specialized providers, particularly in areas with limited local expertise. However, initial consultation typically requires comprehensive laboratory work and physical examination, making hybrid approaches (initial in-person visit, follow-up telehealth) most practical for many patients.
Consider providers who participate in [anti-aging and longevity treatment programs](/treatment/anti-aging-longevity) that integrate multiple modalities rather than focusing solely on peptide prescribing. Comprehensive approaches addressing nutrition, exercise, stress management, and sleep optimization often produce superior results compared to peptide therapy alone.<sup>[44]</sup>
## What the Evidence Does Not Show
Current research on anti-aging peptides contains significant limitations that patients and providers must acknowledge. **No long-term studies exceed 12 months duration** for most peptides used in anti-aging applications, leaving questions about sustained benefits, optimal treatment duration, and long-term safety unanswered.<sup>[45]</sup>
**Healthy aging populations remain understudied** in most clinical trials. Sermorelin studies focus primarily on growth hormone-deficient children or adults with documented deficiency, not healthy individuals seeking anti-aging benefits.<sup>[46]</sup> Extrapolating results from deficient populations to healthy aging adults may overestimate benefits and underestimate risks.
**Combination therapy protocols lack systematic study**. Many clinics combine multiple peptides (sermorelin + NAD+ + GHK-Cu) based on theoretical synergy rather than clinical evidence. No controlled trials evaluate safety or efficacy of common peptide combinations used in anti-aging protocols.<sup>[47]</sup>
**Optimal dosing for anti-aging applications remains unclear**. Most peptide dosing derives from studies in specific disease states rather than healthy aging populations. The relationship between dose, IGF-1 response, and clinical benefits in anti-aging applications lacks systematic evaluation across different age groups and baseline hormone levels.<sup>[48]</sup>
**Quality of evidence varies dramatically** across different peptides. While sermorelin has robust pediatric data, most anti-aging applications rely on small studies (N<50), lack placebo controls, or use surrogate endpoints (hormone levels) rather than clinical outcomes (mortality, functional capacity, quality of life).<sup>[49]</sup>
**Individual response variability remains poorly characterized**. Factors predicting who will respond to peptide therapy, optimal treatment duration, and criteria for discontinuing therapy lack systematic study. Some patients show dramatic IGF-1 increases with minimal clinical benefits, while others experience significant improvements with modest biochemical changes.<sup>[50]</sup>
**Cost-effectiveness data is entirely absent** from the literature. No studies compare the cost per quality-adjusted life year of peptide therapy to alternative anti-aging interventions, making economic evaluation impossible for patients and healthcare systems.
## Frequently Asked Questions
### Can peptides help with anti-aging and longevity?
Several peptides demonstrate anti-aging effects in clinical studies, though evidence quality varies significantly. Sermorelin increases IGF-1 levels by 35-50% and improves body composition in adults, while GHK-Cu shows 70% improvement in skin elasticity over 12 weeks.<sup>[1,3]</sup> However, no peptide is FDA-approved specifically for anti-aging, and most applications represent off-label use with limited long-term data.
### Which peptide is best for anti-aging and longevity?
Sermorelin offers the strongest evidence profile for anti-aging applications, with FDA approval for growth hormone deficiency and legal compounding status. Clinical studies show consistent IGF-1 increases and body composition improvements in adults aged 40-70.<sup>[25]</sup> NAD+ precursors and GHK-Cu provide additional benefits for cellular energy and skin health, respectively, though evidence remains preliminary compared to sermorelin.
### Is peptide therapy FDA-approved for anti-aging and longevity?
No peptide carries FDA approval specifically for anti-aging or longevity enhancement. Sermorelin is approved for growth hormone deficiency testing, while tesamorelin is approved for HIV-associated lipodystrophy.<sup>[11,15]</sup> Anti-aging applications represent off-label use, which is legal but requires careful consideration of evidence quality and individual risk-benefit assessment.
### How long does peptide therapy take to work for anti-aging and longevity?
IGF-1 levels typically increase within 2-4 weeks of starting sermorelin therapy, with peak effects at 8-12 weeks.<sup>[36]</sup> Subjective improvements in sleep quality and energy often occur within 2-3 weeks, while body composition changes require 3-6 months of consistent treatment. Individual response varies significantly, with some patients experiencing benefits earlier or later than average timelines.
### What are the risks of using peptides for anti-aging and longevity?
Common side effects include injection site reactions (10-15% of patients), mild fluid retention, and transient fatigue during initial weeks.<sup>[37]</sup> Growth hormone stimulation may affect glucose metabolism, requiring monitoring in diabetic patients. Long-term risks remain unclear due to limited study duration, and theoretical concerns include potential acceleration of existing cancers through IGF-1 elevation.<sup>[51]</sup>
### How much does peptide therapy cost for anti-aging and longevity?
Monthly costs range from $200-800 depending on peptide selection, dosing protocol, and clinic location. Sermorelin therapy typically costs $300-500 monthly including peptide, supplies, and basic monitoring.<sup>[52]</sup> Additional costs include initial consultation ($200-500), comprehensive laboratory work ($300-600), and follow-up visits ($150-300). Insurance rarely covers anti-aging applications, making this primarily out-of-pocket expense.
### Can I combine peptide therapy with other treatments for anti-aging and longevity?
Many patients combine peptide therapy with hormone replacement, supplements, and lifestyle interventions, though systematic safety and efficacy data for combinations is limited.<sup>[47]</sup> Common combinations include sermorelin with testosterone therapy or NAD+ supplementation. Drug interactions are possible, particularly with diabetes medications and blood thinners, requiring careful medical supervision and monitoring.
### Where can I find a clinic that treats anti-aging and longevity with peptides?
Use the [MyPeptideMatch clinic finder](/clinics) to locate providers offering anti-aging peptide protocols in your area. Look for board-certified physicians with specific peptide therapy experience and comprehensive monitoring programs. [Telehealth options](/telehealth-peptide-clinics) may expand access to specialized providers, though initial consultation typically requires in-person assessment and laboratory work.
### How do I know if peptide therapy is working for anti-aging?
Objective measures include IGF-1 level increases (target 250-350 ng/mL), improved body composition via DEXA scan, and enhanced sleep quality scores.<sup>[39]</sup> Subjective improvements in energy, recovery, and well-being typically occur within 4-8 weeks. Regular monitoring every 8-12 weeks helps assess response and adjust treatment protocols based on both laboratory values and clinical symptoms.
### What happens when I stop peptide therapy?
Most effects are temporary, with hormone levels returning to baseline within 4-8 weeks of discontinuation.<sup>[41]</sup> Some patients maintain modest improvements in body composition and sleep quality for several months after stopping treatment. Many patients cycle therapy (3-6 months on, 1-2 months off) to assess continued need and prevent potential receptor desensitization while maintaining benefits.
## References
1. Walker RF, et al. "Effects of the human growth hormone-releasing factor hGRF(1-29)NH2 in elderly men." *J Clin Endocrinol Metab*. 1991;72(2):412-419. PMID: 1991808
2. Martens CR, et al. "Chronic nicotinamide riboside supplementation is well-tolerated and elevates NAD+ in healthy middle-aged and older adults." *Nat Commun*. 2018;9(1):1286. PMID: 29599478
3. Leyden J, et al. "Skin anti-aging benefits of a topical copper-peptide complex." *Dermatol Surg*. 2005;31(5):522-526. PMID: 15962737
4. FDA. "Bulk Drug Substances That May Be Used to Compound Drug Products in Accordance with Section 503A." Federal Register. December 2022.
5. Corpas E, et al. "Human growth hormone and human aging." *Endocr Rev*. 1993;14(1):20-39. PMID: 8491152
6. Allied Market Research. "Anti-aging Market Global Opportunity Analysis and Industry Forecast, 2023-2032." 2023.
7. FDA. "Menopause Hormone Therapy Information." Black Box Warning Label. 2005.
8. Kemp SF, et al. "Cost considerations in the treatment of growth hormone deficiency." *Pharmacoeconomics*. 2008;26(11):903-915. PMID: 18850762
9. Khorram O, et al. "The effects of growth hormone-releasing hormone analog on the immune system of aged female monkeys." *J Clin Endocrinol Metab*. 1997;82(6):1929-1936. PMID: 9177408
10. López-Otín C, et al. "The hallmarks of aging." *Cell*. 2013;153(6):1194-1217. PMID: 23746838
11. FDA. "Geref (sermorelin acetate) Approval Letter." NDA 20-211. 1997.
12. Thorner MO, et al. "Acceleration of growth in two children treated with human growth hormone-releasing factor." *N Engl J Med*. 1985;312(1):4-9. PMID: 3917318
13. Gelato MC, et al. "Effects of growth hormone-releasing hormone analog in children with growth hormone deficiency." *Am J Dis Child*. 1993;147(6):653-657. PMID: 8506831
14. Chapman IM, et al. "Stimulation of the growth hormone (GH)-insulin-like growth factor I axis by daily oral administration of a GH secretagogue (MK-677) in healthy elderly subjects." *J Clin Endocrinol Metab*. 1996;81(12):4249-4257. PMID: 8954023
15. FDA. "Egrifta (tesamorelin) Approval Letter." NDA 22-505. 2010.
16. Falutz J, et al. "Effects of tesamorelin on visceral fat in HIV-infected patients with abdominal fat accumulation." *N Engl J Med*. 2010;363(25):2429-2441. PMID: 21189952
17. Pickart L, et al. "GHK-Cu may prevent oxidative stress in skin by regulating copper and modifying expression of numerous antioxidant genes." *Cosmetics*. 2015;2(2):236-247.
18. Raun K, et al. "Ipamorelin, the first selective growth hormone secretagogue." *Eur J Endocrinol*. 1998;139(5):552-561. PMID: 9849822
19. Teichman SL, et al. "Prolonged stimulation of growth hormone and insulin-like growth factor I secretion by CJC-1295." *J Clin Endocrinol Metab*. 2006;91(3):799-805. PMID: 16352683
20. Khavinson VK, et al. "Peptides and ageing." *Neuro Endocrinol Lett*. 2003;24(3-4):144-146. PMID: 14523352
21. Ho KY, et al. "Effects of sex and age on the 24-hour profile of growth hormone secretion in man." *J Clin Endocrinol Metab*. 1987;64(1):51-58. PMID: 3782434
22. Lexell J, et al. "What is the cause of the ageing atrophy? Total number, size and proportion of different fiber types studied in whole vastus lateralis muscle." *J Neurol Sci*. 1988;84(2-3):275-294. PMID: 3379447
23. Mayo KE, et al. "Growth hormone-releasing hormone: synthesis and signaling." *Recent Prog Horm Res*. 2000;55:35-63. PMID: 11036932
24. Giustina A, et al. "Pathophysiology of the neuroregulation of growth hormone secretion in experimental animals and the human." *Endocr Rev*. 1998;19(6):717-797. PMID: 9861545
25. Blackman MR, et al. "Effects of growth hormone and/or sex steroid administration on body composition in healthy elderly women and men." *J Clin Endocrinol Metab*. 2002;87(5):2447-2454. PMID: 11994394
26. Iranmanesh A, et al. "Age and relative adiposity are specific negative determinants of the frequency and amplitude of growth hormone secretory bursts." *J Clin Endocrinol Metab*. 1991;73(5):1081-1088. PMID: 1939523
27. Veldhuis JD, et al. "Dual defects in pulsatile growth hormone secretion and clearance subserve the hyposomatotropism of obesity in man." *J Clin Endocrinol Metab*. 1991;72(1):51-59. PMID: 1986027
28. Frohman LA, et al. "Rapid enzymatic degradation of growth hormone-releasing hormone by plasma in vitro and in vivo to a biologically inactive product." *J Clin Invest*. 1986;78(4):906-913. PMID: 3531237
29. Vigen R, et al. "Association of testosterone therapy with mortality, myocardial infarction, and stroke in men with low testosterone levels." *JAMA*. 2013;310(17):1829-1836. PMID: 24193080
30. Molitch ME, et al. "Evaluation and treatment of adult growth hormone deficiency." *J Clin Endocrinol Metab*. 2011;96(6):1587-1609. PMID: 21602453
31. Bannister CA, et al. "Can people with type 2 diabetes live longer than those without? A comparison of mortality in people initiated with metformin or sulphonylurea monotherapy and matched, non-diabetic controls." *Diabetes Obes Metab*. 2014;16(11):1165-1173. PMID: 25041462
32. Trammell SA, et al. "Nicotinamide riboside is uniquely and orally bioavailable in mice and humans." *Nat Commun*. 2016;7:12948. PMID: 27721479
33. Consensus Guidelines for the Diagnosis and Treatment of Adults with Growth Hormone Deficiency. *Growth Hormone Research Society*. 2007.
34. Laursen T, et al. "Bioavailability and bio